





Wolff-Parkinson-White Syndrome: When Your Heart Has a Secret Shortcut
Wolff-Parkinson-White syndrome is a congenital heart condition caused by an extra electrical pathway in the heart that bypasses normal conduction, potentially triggering episodes of abnormally rapid heartbeat. Many people with WPW are diagnosed incidentally on a routine ECG before any symptoms appear. Others experience sudden palpitations, dizziness, or breathlessness. Management ranges from careful monitoring to medications to catheter ablation, a minimally invasive procedure that can eliminate the accessory pathway. WPW is not rare, but it is well understood and highly treatable. A specialist evaluation is the essential first step toward informed, confident management of this condition.
AT A GLANCE
Wolff-Parkinson-White (WPW) syndrome is a congenital heart condition in which an extra electrical pathway connects the upper and lower chambers of the heart, bypassing the normal conduction system. This "accessory pathway" can trigger episodes of abnormally fast heart rhythms — sometimes dramatic, sometimes silent. WPW affects people of all ages and is often discovered incidentally on a routine ECG. While many people with WPW live normally for years without knowing they have it, some experience disabling or even dangerous arrhythmias. Understanding this condition is the first step toward living confidently with it.
WHAT IS WOLFF-PARKINSON-WHITE SYNDROME?
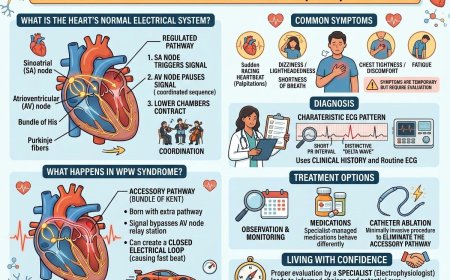
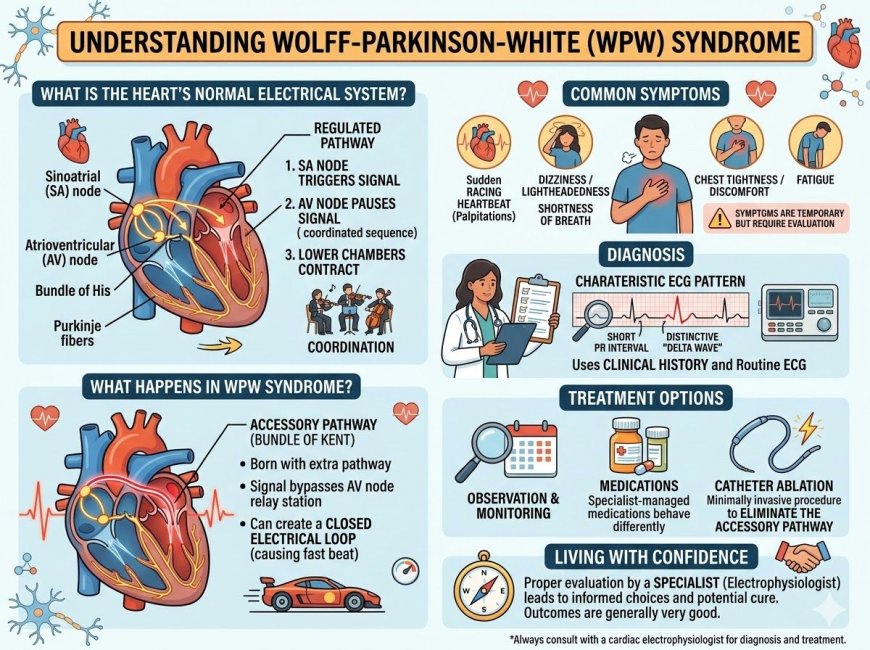
Your heart runs on electricity. Every heartbeat is triggered by an electrical signal that travels along a carefully regulated pathway — starting at the top of the heart, pausing briefly at a relay station called the AV node, and then continuing downward to cause the lower chambers to contract.
This built-in pause is not a flaw. It is your heart's way of ensuring the upper and lower chambers work in coordinated sequence — like a conductor keeping two sections of an orchestra in time.
In Wolff-Parkinson-White syndrome, a person is born with an additional electrical pathway — called an accessory pathway or bundle of Kent — that bypasses this relay station entirely. The signal can travel down this shortcut faster than normal, or — more problematically — travel back up it in the wrong direction, creating a closed electrical loop that causes the heart to beat very rapidly.
This type of abnormally fast rhythm is called a supraventricular tachycardia (SVT), and in WPW, a specific form called atrioventricular reentrant tachycardia (AVRT) is most common. Less commonly, in certain individuals, the accessory pathway can conduct a more dangerous arrhythmia involving the upper chambers, which is why WPW is taken seriously even in people who feel well.
WHO IS AFFECTED?
WPW is present from birth — it is a structural variation that develops in the womb. It is not caused by lifestyle, diet, age, or anything you did or didn't do.
It is estimated to affect roughly 1 to 3 in every 1,000 people in the general population, though actual numbers may be higher because many individuals are never diagnosed.
Those more likely to receive a WPW diagnosis include:
- People who experience unexplained episodes of racing heartbeat, especially in childhood or early adulthood
- Individuals identified on a routine ECG — often before any symptoms have appeared
- Those with a family history of WPW or unexplained arrhythmias
- People with certain other congenital heart conditions, particularly Ebstein's anomaly, which has a known association with WPW
WPW can affect infants, children, teenagers, and adults. Symptoms may first appear at any point in life. Some people are diagnosed in their 20s or 30s; others not until much later when a routine medical check captures the telltale ECG pattern.
SYMPTOMS & WARNING SIGNS
What WPW can feel like
The most characteristic symptom of WPW is a sudden onset of rapid heartbeat — sometimes described as the heart suddenly "racing," "fluttering," or "pounding." These episodes can come on without warning and typically stop just as abruptly.
During an episode, a person may experience:
- A sensation of the heart beating very fast, sometimes 150 to 250 beats per minute
- Palpitations — a strong awareness of the heartbeat
- Dizziness or lightheadedness
- Shortness of breath
- Chest tightness or discomfort
- Fatigue during or after the episode
- In some cases, fainting (syncope) or near-fainting (presyncope)
What gets ignored — and why it matters
Many people dismiss these episodes. "I must be stressed." "I had too much coffee." "It stopped on its own, so it's probably nothing."
This is understandable. Episodes of WPW-related tachycardia often do resolve on their own in minutes. But dismissing them means delaying a diagnosis — and WPW is a condition that benefits significantly from proper evaluation and, where appropriate, treatment.
WPW on ECG — the silent finding
A significant number of people with WPW are diagnosed not because of symptoms, but because their ECG shows the characteristic pattern: a short PR interval and a distinctive "delta wave" — the fingerprint of early ventricular activation via the accessory pathway. If you have been told your ECG shows something unusual, this warrants a conversation with a specialist.
THE GENERAL TREATMENT LANDSCAPE
There is no single approach that applies to every person with WPW. Management decisions depend on many individual factors: whether you have symptoms, the nature of any arrhythmias you experience, the properties of your accessory pathway, your age, your activity level, and your personal preferences and risk tolerance.
Observation and monitoring
For individuals with WPW detected incidentally on ECG who have never had symptoms, some cardiologists and electrophysiologists may recommend a period of careful observation, monitoring, and risk assessment. This is not the same as dismissal — it involves understanding the pathway and its potential behavior.
Medications
There are categories of medications used in cardiology to help control heart rhythm and rate. These are not used in the same way in all patients with WPW, and some medications that are commonly used for other arrhythmias behave differently — and can be problematic — in WPW. This is an important reason why WPW should be managed by a specialist who understands its specific electrical characteristics.
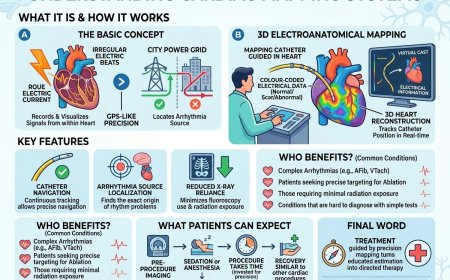
Catheter Ablation
Catheter ablation is a procedure that has transformed the management of WPW for many patients. In general terms, it involves passing thin, flexible tubes (catheters) through blood vessels to reach the heart, mapping the electrical pathways, and then applying energy — most commonly radiofrequency energy — to the precise location of the accessory pathway to eliminate it.
For many individuals, particularly those with symptomatic arrhythmias, catheter ablation offers the possibility of eliminating the underlying cause of the problem rather than simply managing symptoms. The decision to pursue ablation is an individual one that your electrophysiologist will discuss with you based on your specific circumstances.
Your cardiologist or electrophysiologist will determine which approach — or combination of approaches — is most appropriate for your individual situation.
QUESTIONS TO ASK YOUR DOCTOR
If you have been diagnosed with WPW, or if your ECG has been flagged as unusual, these are the kinds of questions that can help you have a more informed conversation with your specialist:
- What does my ECG finding mean in practical terms — and does it require treatment?
- Have I been referred to an electrophysiologist (a specialist in heart rhythm)?
- What is the difference between my options — observation, medication, and ablation?
- Are there activities, sports, or situations I should be aware of while my condition is being evaluated?
- What symptoms should prompt me to seek immediate care?
- Is an electrophysiology study (EPS) recommended in my case to better understand the pathway?
- What happens if I choose not to treat — what does monitoring look like?
- Do any of my family members need to be evaluated?
You deserve clear, individualized answers — not general reassurances. A specialist second opinion is always your right.
COMMON MISCONCEPTIONS
"It's just an irregular heartbeat — everyone gets those." Palpitations are common, but WPW is a specific structural condition with a distinct electrical signature. It is not the same as occasional benign palpitations and deserves proper evaluation.
"The ECG was abnormal but my doctor said not to worry." Not all WPW carries the same risk, and some presentations are genuinely low-risk. But "don't worry" is not the same as "it's been properly evaluated by a specialist." An electrophysiologist is the right person to make that determination.
"Catheter ablation is major surgery." It is not open-heart surgery. Catheter ablation is a minimally invasive procedure performed through blood vessels. Many patients return home the same day or within 24 hours. Your electrophysiologist can walk you through exactly what to expect.
"If I've lived with it this long without problems, I must be fine." Many people with WPW do very well for years. But the properties of accessory pathways can change over time, and a baseline evaluation with a specialist ensures you are making an informed choice rather than an uninformed assumption.
"It's a rare, exotic condition." WPW is not rare. It affects a meaningful proportion of the population. It has been well understood and well studied for decades. Treatment options are established, and outcomes for well-managed WPW are generally very good.
PROFESSIONAL SUPPORT SECTION
If you have been diagnosed with Wolff-Parkinson-White syndrome, have noticed episodes of rapid or irregular heartbeat, or have been told your ECG shows an unusual pattern, speaking with a qualified cardiologist or cardiac electrophysiologist is the right next step.
Connect with experienced U.S.-based cardiac specialists for a comprehensive consultation. They will carefully review your case and help determine the most appropriate next steps for your individual health needs:
👉 https://myamericandoctor.com/our-doctors/
You may also choose to enroll in our upcoming concierge medical clinic in India, Global Concierge Doctors. We offer U.S.-style primary care with 24/7 access to India-based physicians for ongoing guidance on any heart health concern. When required, we coordinate referrals to trusted cardiac specialists in India and the U.S. for advanced evaluation and care.
Your heart health decisions today shape your life tomorrow.
FINAL WORD
Living with WPW — whether you've known about it for years or were just told about it last week — can feel unsettling. A condition you were born with. A part of your heart's wiring that most people will never have.
But WPW is also one of the most treatable cardiac conditions there is. The knowledge about it is mature. The evaluation tools are precise. The treatment options — including ablation — have helped many people go on to live entirely normal, unrestricted lives.
The most important thing you can do is get properly evaluated by the right specialist. Not to be frightened. Not to be rushed into anything. But to understand exactly what you are dealing with — and to make an informed, empowered choice about how to manage it.
Your heart has been beating faithfully, extra pathway and all, for your entire life. Now let's make sure it gets the attention it deserves.
READER POLL
Have you or someone you know been diagnosed with WPW or an arrhythmia?
- Yes, and I've been treated
- Yes, but I'm still figuring out next steps
- I've had symptoms but no diagnosis yet
- No, but I found this article helpful
Share this article with someone who may have experienced unexplained heart palpitations.
MEDICAL DISCLAIMER
The information in this article is intended for general educational purposes only and does not constitute medical advice, diagnosis, or treatment. References to ECG findings, catheter ablation, electrophysiology studies, accessory pathways, medications, or any cardiac condition or procedure are for informational purposes only and are not recommendations for specific tests, treatments, or interventions.
Not a Recommendation for Specific Tests or Treatments. This content does not recommend or endorse any specific cardiac diagnostic procedure, device, medication, or intervention. All decisions regarding cardiac care — including whether to pursue evaluation, monitoring, medication, or ablation — must be made in consultation with a qualified physician who has reviewed your individual medical history, symptoms, test results, and clinical circumstances.
The statistics and clinical information cited in this article are drawn from published medical literature and public health sources available at the time of writing. Medical science evolves continuously, and information may change.
Seek immediate emergency medical attention if you experience chest pain, fainting, severe shortness of breath, or a prolonged episode of very rapid heartbeat that does not resolve.
This content was developed with AI-assisted research and editorial support and reviewed under Dr. Deepak Thomas's editorial guidelines for MyAmericanDoctor.com.
Category: Cardiology
SOURCES
-
Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia. Journal of the American College of Cardiology. 2016;67(13):e27–e115.
-
Wolff L, Parkinson J, White PD. Bundle-branch block with short P-R interval in healthy young people prone to paroxysmal tachycardia. American Heart Journal. 1930;5(6):685–704. (Original description)
-
Al-Khatib SM, Pritchett EL. Clinical features of Wolff-Parkinson-White syndrome. American Heart Journal. 1999;138(3):403–413.
-
Pappone C, Vicedomini G, Manguso F, et al. Wolff-Parkinson-White syndrome in the era of catheter ablation. Circulation. 2014;130(10):811–819.
-
Etheridge SP, Escudero CA, Blaufox AD, et al. Life-threatening event risk in children with Wolff-Parkinson-White syndrome: A multicenter international study. JACC: Clinical Electrophysiology. 2018;4(4):433–444.
-
Brugada J, Katritsis DG, Arbelo E, et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardia. European Heart Journal. 2020;41(5):655–720.
-
American Heart Association. Wolff-Parkinson-White Syndrome. www.heart.org
What's Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Angry
0
Angry
0
 Sad
0
Sad
0
 Wow
0
Wow
0