





When Medications Aren't Enough: A Complete Guide to AFib Catheter Ablation
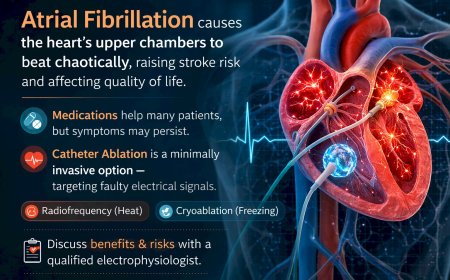
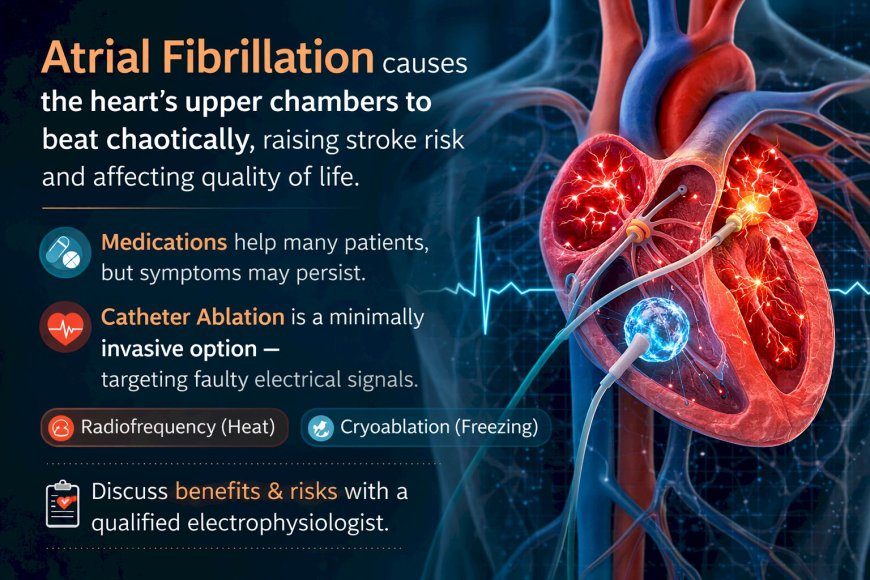
Atrial fibrillation causes the heart's upper chambers to beat chaotically, raising stroke risk and affecting quality of life. While medications help many patients, some continue to experience symptoms despite medical therapy. For these patients, catheter ablation offers an established minimally invasive option — targeting the faulty electrical signals, most commonly through pulmonary vein isolation. This can be achieved via radiofrequency (heat) or cryoablation (freezing), with the choice guided by individual factors and specialist assessment. Like any cardiac procedure, ablation carries both benefits and risks that must be discussed with a qualified electrophysiologist. This article is for education only — consult a specialist for decisions specific to your situation.
At A Glance
Atrial fibrillation affects millions of people worldwide, causing an irregular, often rapid heartbeat that disrupts daily life and raises the risk of stroke. For many patients, medications help manage symptoms — but for others, they don't provide adequate relief. Catheter ablation is a procedure that offers another path forward. This article explains what AFib is, why ablation is used, what the procedure involves, its general benefits and risks, and the questions every patient should be asking their cardiologist before making any decision.
The Heartbeat That Won't Behave
You noticed it first during an ordinary Tuesday morning. A fluttering in your chest. A strange racing sensation that came out of nowhere, lasted a few minutes, then disappeared as suddenly as it arrived. You told yourself it was stress. Too much coffee. A bad night's sleep.
Then it happened again. And again.
Your doctor put you on medication. It helped for a while. But the episodes kept coming — sometimes less frequent, sometimes more. You're now on your second medication adjustment, and your cardiologist has started talking about something called catheter ablation.
And you have no idea what to make of it.
Sound familiar?
You're not alone. And the fact that you're reading this means you're taking the right step — understanding your options before making a decision that involves your heart.
What Is Atrial Fibrillation?
The heart runs on electrical signals. In a healthy heart, these signals originate from a specific point and travel in an orderly sequence, causing the heart to contract and pump blood in a coordinated rhythm.
In atrial fibrillation — commonly called AFib — this electrical system misfires. Instead of one clean signal, the upper chambers of the heart (the atria) receive chaotic, disorganised electrical impulses. The result: the atria quiver rather than contract properly, and the heart's pumping becomes irregular and often rapid.
AFib is not a single, uniform condition. It can be occasional (paroxysmal), persistent, or long-standing persistent. Some people feel it intensely. Others have no symptoms at all and discover it only during a routine check-up. This variability is one of the reasons AFib can be difficult to manage and why treatment is not one-size-fits-all.
Why AFib Matters Beyond the Symptoms
Beyond the palpitations, breathlessness, and fatigue that many AFib patients experience, the condition carries a significant concern: the irregular rhythm in the atria can allow blood to pool and form clots, particularly in a small pouch of the heart called the left atrial appendage. If a clot travels to the brain, it causes a stroke.
This is why most patients with AFib are kept on blood thinners — also called anticoagulants — to reduce the risk of stroke. These medications do not correct the heart rhythm, but they play a critical role in protecting against one of AFib's most serious complications.
This is why AFib is taken seriously by cardiologists even in patients who feel relatively well. It is not just about comfort — it is about long-term risk.
How AFib Is Usually Managed First
When AFib is diagnosed, cardiologists typically consider several broad approaches. These generally fall into categories — managing the heart rate, attempting to restore and maintain normal rhythm, and reducing stroke risk. Medications are often the first step in most of these areas.
For many patients, medications work well. Symptoms reduce. Quality of life improves. The condition is managed.
But medications are not the right answer for everyone. Some patients continue to have significant symptoms despite trying multiple medications. Some experience side effects that affect their daily lives. Some have AFib that recurs frequently despite medical therapy. And some simply want a treatment that addresses the underlying electrical problem more directly.
This is where catheter ablation enters the conversation.
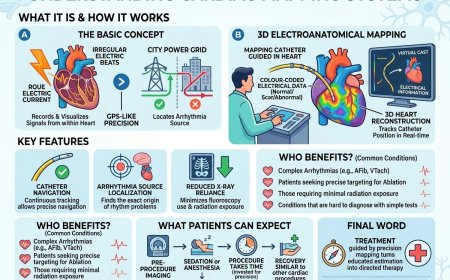
What Is Catheter Ablation?
Catheter ablation is a procedure used to treat abnormal heart rhythms by targeting and modifying the specific areas of heart tissue responsible for generating the faulty electrical signals.
The word "ablation" comes from the Latin for "removal." In cardiac ablation, tissue is not surgically removed — instead, it is rendered electrically inactive through the application of energy. The two most common energy types used in AFib ablation are radiofrequency energy (which uses heat) and cryoenergy (which uses freezing). Both aim to achieve the same goal through different means.
The procedure is performed by an electrophysiologist — a cardiologist who specialises in the heart's electrical system.
What Is Pulmonary Vein Isolation?
In the majority of AFib cases, the faulty electrical signals that trigger the irregular rhythm originate from areas near the pulmonary veins — the four veins that carry oxygenated blood from the lungs into the left atrium.
Pulmonary vein isolation (PVI) is the cornerstone of most AFib ablation procedures. The goal is to create a barrier of scar tissue around the openings of the pulmonary veins, electrically isolating them from the rest of the atrium so their erratic signals can no longer trigger AFib.
PVI is not a new concept — it has been performed and refined over many years and is now the standard target for most AFib ablation procedures, regardless of whether radiofrequency or cryoenergy is used.
Radiofrequency Ablation vs. Cryoablation: Two Paths to the Same Goal
Both radiofrequency (RF) ablation and cryoablation are established techniques for performing pulmonary vein isolation. They differ in the type of energy used and the way that energy is delivered.
Radiofrequency Ablation
RF ablation uses heat energy delivered through the tip of a catheter. The electrophysiologist carefully maps the heart's electrical activity in real time using sophisticated 3D mapping systems, then applies radiofrequency energy point by point to create the isolation line around the pulmonary veins. This approach allows a high degree of precision and flexibility — the physician can adapt the ablation pattern based on what the mapping reveals.
Cryoablation
Cryoablation uses extreme cold rather than heat. A specialised balloon catheter is positioned at the opening of each pulmonary vein, inflated to create contact, and then cooled to very low temperatures to freeze and scar the tissue, achieving isolation. The balloon approach is designed to isolate each pulmonary vein in a single, circular application rather than point by point.
Which Is Better?
This is one of the most common questions patients ask — and it is genuinely a question for your electrophysiologist, not this article.
Both techniques are well-established. Both are used widely by experienced electrophysiologists. The choice between them depends on factors including the anatomy of your pulmonary veins, the nature of your AFib, the experience and preference of your physician, and the specific facilities available. Neither is universally superior — what matters most is that the procedure is performed by an experienced specialist in an appropriate setting.
What Happens During a Catheter Ablation Procedure?
Without going into technical clinical detail, here is a general overview of what a catheter ablation procedure involves — so that you are not walking into the experience without any understanding of what to expect.
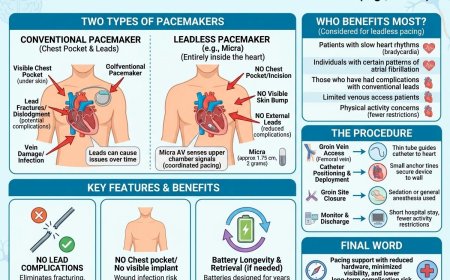
The procedure is performed in a specialised cardiac laboratory. Patients typically receive sedation or general anaesthesia so they are comfortable throughout. Access to the heart is usually achieved through catheters — thin, flexible tubes — inserted through a vein in the groin area and guided to the heart under imaging guidance.
Once inside the heart, the electrophysiologist uses mapping technology to create a detailed picture of the heart's electrical activity and anatomy. The ablation energy is then delivered to the targeted areas. The entire procedure typically takes several hours, though this varies depending on the complexity of the case.
After the procedure, patients are monitored for a period of time before being discharged, which may be the same day or the following day depending on individual circumstances.
Who Might Be Considered for AFib Ablation?
Catheter ablation is not appropriate for every AFib patient. The decision involves careful evaluation by an electrophysiologist. Generally speaking, ablation tends to be considered in situations such as:
- Patients who continue to have significant AFib symptoms despite appropriate medical therapy
- Patients who cannot tolerate the side effects of rhythm control medications
- Patients for whom restoring and maintaining normal rhythm is a clinical priority
- Certain patients in whom early rhythm control may be especially beneficial
The type of AFib — whether it is paroxysmal, persistent, or long-standing persistent — also plays an important role in the decision, as does the presence of other heart conditions, overall health, and the patient's own preferences and quality-of-life goals.
This list is not a checklist for self-assessment. Every individual case is different. These are general considerations that your cardiologist and electrophysiologist will weigh together with your complete clinical picture.
General Benefits of Catheter Ablation
The potential benefits of catheter ablation for AFib, as understood from the body of medical evidence, include:
- Reduction or elimination of AFib episodes in appropriately selected patients
- Improvement in symptoms such as palpitations, breathlessness, and fatigue
- Potential improvement in quality of life
- For some patients, reduction in the need for long-term rhythm control medication
- The possibility of a more durable restoration of normal rhythm compared to medication alone in certain patient groups
It is important to understand that ablation does not guarantee a permanent cure. AFib can recur after ablation, sometimes requiring a repeat procedure or continued medication. The likelihood of a successful outcome depends on many individual factors that your electrophysiologist is best placed to discuss with you.
General Risks and Considerations
Like any invasive cardiac procedure, catheter ablation carries risks. These are generally considered in the context of the risks of untreated or inadequately controlled AFib — but they are real and must be understood before proceeding. General categories of risk include:
- Risks associated with vascular access (the entry point for the catheters)
- Risk of bleeding or blood vessel injury
- Risk of damage to adjacent cardiac structures
- Risk of fluid accumulation around the heart (pericardial effusion)
- Small risk of stroke or transient ischaemic attack, despite anticoagulation measures taken during the procedure
- Risks associated with anaesthesia
- The possibility that the procedure does not achieve the desired result, or that AFib recurs
This is not a complete list, and individual risk profiles vary significantly. A thorough discussion of risks and benefits specific to your situation with your electrophysiologist is an essential part of any decision-making process.
Recovery: What to Generally Expect
Recovery from catheter ablation varies between individuals. Most patients are monitored in hospital for a period following the procedure. There is typically a recovery period during which physical activity is restricted. It is common for patients to experience some irregular heartbeats in the weeks following ablation — this does not necessarily mean the procedure has failed, as the treated tissue takes time to stabilise. Most patients are advised to continue certain medications for a period after the procedure.
The timeline for returning to normal activities, and the follow-up schedule, will be guided by your individual clinical team.
Questions to Ask Your Electrophysiologist
Rather than arriving at your consultation uncertain and overwhelmed, consider bringing these questions:
- Am I a good candidate for ablation given my type of AFib and my overall health?
- Which technique — radiofrequency or cryoablation — would you recommend for me, and why?
- What is your personal experience and volume with this procedure?
- What is a realistic expectation of outcome for someone in my situation?
- What are the specific risks I should be aware of given my individual health history?
- What happens if the procedure doesn't work, or if my AFib returns?
- What medications will I need to continue after the procedure?
- What does the recovery process look like for me specifically?
- Can I come off of anticoagulants after ablation? For most patients, the answer is no. Ablation restores rhythm but does not eliminate the underlying stroke risk associated with AFib. Your cardiologist will assess your individual stroke risk — typically using a scoring tool called CHA₂DS₂-VASc — to determine whether anticoagulation should continue regardless of ablation outcome. Do not stop blood thinners without explicit guidance from your specialist.
These are your questions to ask. Our specialists at MyAmericanDoctor are available to help you understand the answers — and to offer a second perspective if you need one.
Common Misconceptions About AFib Ablation
"Ablation means open-heart surgery" It does not. Catheter ablation is a minimally invasive procedure performed through catheters — there is no surgical incision into the chest.
"If medication isn't working, nothing will" Not accurate. Ablation addresses the electrical source of the problem in a way that medications cannot. It is a different category of treatment, not simply a stronger medication.
"Ablation is a last resort" The timing of when ablation is considered varies and is evolving. For some patients and some types of AFib, it may be considered earlier in the treatment pathway. This is a conversation for your cardiologist.
"One ablation will fix AFib permanently" Not always. AFib may recur, and some patients require more than one procedure. This does not mean the first procedure failed — it reflects the complex, progressive nature of the condition in some individuals.
"I'm too old for ablation" Age alone is not a disqualifying factor. The decision is based on overall health, the nature of the AFib, and a careful benefit-risk assessment by your specialist.
Professional Support Options
If your doctor has recommended catheter ablation, you have been diagnosed with AFib, or you want a specialist second opinion before making any decision, our cardiac specialists are here to help.
Connect with experienced U.S.-based cardiac specialists for a comprehensive consultation. They will carefully review your individual case and help you understand your options:
👉 https://myamericandoctor.com/our-doctors/
You may also choose to enroll in our upcoming concierge medical clinic in India, Global Concierge Doctors. We offer U.S.-style primary care with 24/7 access to India-based physicians for ongoing guidance on any health concern. When required, we coordinate referrals to trusted cardiac specialists in India and the U.S. for advanced evaluation and care.
Your heart health decisions today shape your life tomorrow.
The Final Word
AFib is a condition that demands to be taken seriously — not because it is automatically dangerous in every case, but because left unmanaged, it carries real long-term risks. Medications are a valuable tool. And for those for whom medications aren't enough, catheter ablation represents a well-established, thoughtfully performed procedure that has helped many patients reclaim a normal rhythm and a better quality of life.
The decision about whether ablation is right for you is not one to make based on an article. It is one to make in conversation with a specialist who knows your heart, your history, and your goals.
You now have the vocabulary to have that conversation. Use it.
Reader Poll
Has your cardiologist discussed catheter ablation with you?
- Yes, and I want to understand it better before deciding
- Yes, and I've already had the procedure
- No, but I'm curious if I might be a candidate
- I'm managing my AFib with medication and it's working well
Share This Article
Know someone living with AFib who is confused about their treatment options? Share this article — understanding the landscape of what's available is the first step to having an informed conversation with their doctor.
Medical Disclaimer
This article is provided strictly for educational, informational, and awareness purposes only. The content is intended as a general overview of atrial fibrillation and catheter ablation procedures and does not constitute professional medical advice, diagnosis, treatment, or a substitute for consultation with qualified healthcare professionals.
No Doctor-Patient Relationship
The information presented in this article does not establish a doctor-patient relationship between the reader and the author, publisher, or any affiliated entities. No medical decisions should be made based solely on the content of this article.
Consult Qualified Medical Professionals
If you have been diagnosed with atrial fibrillation, are experiencing cardiac symptoms, or have concerns about heart rhythm, seek consultation with a qualified cardiologist or electrophysiologist. For medical emergencies, contact emergency services immediately.
Individual Medical Situations Vary
Every person's cardiac condition, health history, risk factors, and circumstances are unique. Treatment decisions, including whether catheter ablation is appropriate, must be made in direct consultation with licensed healthcare providers who have access to your complete medical history and can perform a proper clinical evaluation.
Not a Recommendation for Specific Tests or Treatments
References to catheter ablation, pulmonary vein isolation, radiofrequency ablation, cryoablation, medications, or any other cardiac procedure or treatment in this article are for informational purposes only and do not constitute a recommendation that you should or should not undergo any specific procedure or treatment.
No Guarantee of Accuracy or Completeness
While efforts have been made to provide accurate information, medical knowledge evolves continuously, particularly in the field of cardiac electrophysiology. The information in this article may not reflect the most current research, clinical guidelines, or medical practices.
Do Not Disregard or Delay Professional Medical Advice
Never disregard or delay seeking professional medical advice because of something you have read in this article. Always discuss your specific situation with your personal cardiologist or electrophysiologist.
Limitation of Liability
To the fullest extent permitted by law, the author, publisher, and affiliated entities disclaim all liability for any direct, indirect, incidental, consequential, or punitive damages arising from the use of, or reliance on, information contained in this article.
Acknowledgment
By reading this article, you acknowledge that it has been created with the assistance of artificial intelligence. While every effort has been made to ensure accuracy, readers are strongly encouraged to consult qualified healthcare professionals and refer to peer-reviewed medical literature before making any health-related decisions.
Sources Consulted
The following peer-reviewed publications, clinical guidelines, and authoritative medical resources were referenced in the preparation of this article:
- January CT, et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation. Journal of the American College of Cardiology. 2019;74(1):104–132.
- Hindricks G, et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation. European Heart Journal. 2021;42(5):373–498.
- Calkins H, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation. Heart Rhythm. 2017;14(10):e275–e444.
- Packer DL, et al. Cryoablation versus Radiofrequency Ablation for Paroxysmal Atrial Fibrillation (STOP AF First Trial). New England Journal of Medicine. 2021;384(4):305–315.
- Haïssaguerre M, et al. Spontaneous Initiation of Atrial Fibrillation by Ectopic Beats Originating in the Pulmonary Veins. New England Journal of Medicine. 1998;339(10):659–666. (The foundational paper establishing pulmonary vein isolation as the cornerstone of AFib ablation.)
- Andrade JG, et al. Cryoablation or Drug Therapy for Initial Treatment of Atrial Fibrillation (EARLY-AF Trial). New England Journal of Medicine. 2021;384(4):316–324.
- American Heart Association — Atrial Fibrillation Patient Resources. heart.org
- European Heart Rhythm Association (EHRA) Patient Information on Catheter Ablation. escardio.org
- Heart Rhythm Society — Patient Resources: Catheter Ablation for AFib. hrsonline.org
- Noseworthy PA, et al. Atrial Fibrillation Burden and the Risk of Stroke. Circulation. 2018;137(20):2118–2125.
Last Updated: 8th March 2026
What's Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Angry
0
Angry
0
 Sad
0
Sad
0
 Wow
0
Wow
0