





What Are Targeted Therapies? Understanding Precision Cancer Medicine
Targeted therapy represents a revolutionary shift in cancer treatment, attacking specific cancer cell vulnerabilities while sparing healthy tissue. Unlike traditional chemotherapy that kills all rapidly dividing cells, targeted therapies use drugs designed to interfere with specific molecules that drive cancer growth. This precision approach offers better outcomes with fewer side effects, but confusion and fear keep many patients from accessing these life-saving treatments. Understanding how targeted therapies work, who qualifies, and when to consider them could be the difference between aggressive disease progression and long-term control.

The Diagnosis That Changes Everything
Your oncologist just told you about your treatment plan. Surgery, yes. Radiation, maybe. Chemotherapy, probably. But then they mentioned something else: "targeted therapy." Or was it "precision medicine"? You nodded like you understood, but you walked out of that office confused and terrified.
Sound familiar?
You've been googling non-stop. One website says targeted therapy is "revolutionary." Another warns about "expensive designer drugs with no guarantees." Your neighbor's cousin tried it and it worked miracles. Your uncle's friend said it didn't work at all. And meanwhile, your cancer isn't waiting for you to figure this out.
Here's the truth: targeted therapy isn't some futuristic experimental treatment. It's already saving lives. But the confusion around what it is, how it works, and who should get it is literally costing patients years of life they could have had.
Let me be very direct: if your doctor mentioned targeted therapy as an option and you dismissed it because you didn't understand it, you need to read every word of this article.
Why Your Brain Is Protecting You to Death
Your mind is playing a dangerous game right now. It's called optimism bias, and it's affecting cancer patients every single day.
"Targeted therapy sounds complicated. I'll just stick with regular chemo."
"My cancer isn't that special."
"If it was really important, my doctor would have insisted."
These thoughts feel logical. They feel safe. They're actually your brain's way of avoiding the hard work of understanding something new when you're already overwhelmed.
While you're busy convincing yourself that standard treatment is "good enough," your cancer cells might have specific vulnerabilities that targeted therapy could exploit. Vulnerabilities that chemotherapy alone won't touch effectively.
What Targeted Therapy Actually Is (Without the Medical Jargon)
Imagine your cancer as a city of criminal cells. Traditional chemotherapy is like carpet bombing the entire city — it kills the criminals, but it also destroys schools, hospitals, and homes. Targeted therapy is like a precision strike team that identifies the criminals by their unique tattoos and takes them out specifically.
Here's how it really works:
Standard Chemotherapy: Attacks all rapidly dividing cells. It cannot distinguish between cancer cells and healthy cells that naturally divide quickly — such as hair follicles, the digestive tract lining, and bone marrow. It kills cancer but damages healthy tissue, which is the source of its well-known side effects.
Targeted Therapy: Identifies specific mutations or proteins unique to your cancer cells. It attacks only cells with those specific markers, leaving most healthy cells unaffected. Side effects are often fewer and different in character because healthy cells are not the primary target.
What You're Telling Yourself: "It's just another type of chemo with a fancy name."
The Reality: Targeted therapy is fundamentally different. It's not about poisoning fast-growing cells. It's about exploiting specific weaknesses in your particular cancer's biology.
The Science Your Oncologist Assumed You Understood
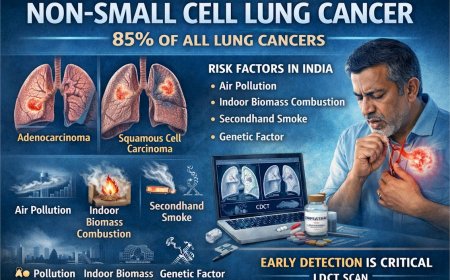
Cancer isn't one disease. Your breast cancer is different from your neighbor's breast cancer at the molecular level. Your lung cancer has different mutations than another patient's lung cancer.
Targeted therapies work because they attack these specific differences:
HER2-Positive Breast Cancer: Some breast cancers have too much of a protein called HER2 on their surface. This makes them grow aggressively. Targeted drugs like trastuzumab (Herceptin) block HER2, stopping the cancer's growth signals.
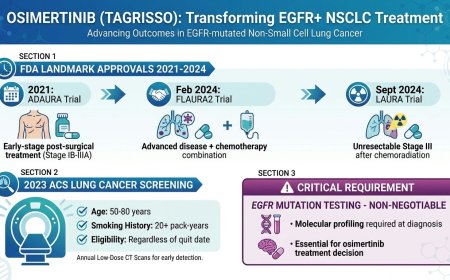
EGFR-Mutated Lung Cancer: Certain lung cancers have mutations in a gene called EGFR. These mutations tell cancer cells to grow non-stop. Targeted drugs like erlotinib or osimertinib block this signal.
BRAF-Mutated Melanoma: Some melanomas have a BRAF mutation that drives rapid growth. Drugs like vemurafenib target this specific mutation.
BCR-ABL Chronic Myeloid Leukemia: This blood cancer has a specific genetic abnormality. Drugs like imatinib (Gleevec) specifically attack cells with this abnormality.
Real Patient Story: Priya's Second Chance
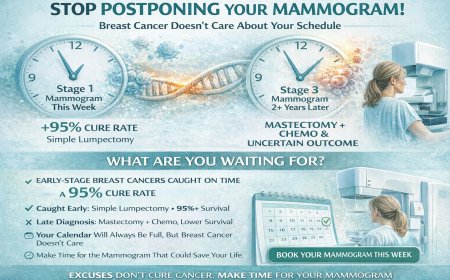
Priya, a 52-year-old teacher from Mumbai, was diagnosed with stage 3 HER2-positive breast cancer. Her oncologist recommended chemotherapy plus targeted therapy (trastuzumab).
Her doctor explained: "Without trastuzumab, your chance of recurrence within five years is significantly higher. With it, we can potentially reduce that risk substantially. For your specific cancer type, this isn't an optional addition — it is a core part of treatment."
Priya started the combined treatment. Three years later, she's cancer-free. Her neighbor, who had the same diagnosis but skipped the targeted therapy, had a recurrence within 18 months.
The uncomfortable reality: skipping a recommended targeted therapy to reduce treatment burden can result in recurrence that requires far more intensive — and prolonged — treatment, with uncertain outcomes.
How Doctors Decide If Targeted Therapy Is Right for You
This isn't a decision your doctor makes based on how "bad" your cancer looks or how you feel. It's based on science.
Step 1: Biomarker Testing
Your tumor is tested for specific genetic mutations or protein overexpression. This is done through:
Immunohistochemistry (IHC) testing, Fluorescence in situ hybridization (FISH) testing, and Next-generation sequencing (NGS) genetic testing.
Step 2: Matching Mutations to Drugs
If your tumor has a mutation with a corresponding targeted therapy, you're a candidate. It's that simple.
Step 3: Evaluating Your Overall Health
Some targeted therapies have specific side effects. Your doctor ensures you can tolerate them.
What You Need to Know: Not every cancer has a targetable mutation. Not every mutation has a corresponding drug. But if your cancer does, and a drug exists, refusing it because you don't understand it is like refusing insulin for diabetes because you don't understand how it regulates blood sugar.
The Types of Targeted Therapies (What They Actually Do)
Monoclonal Antibodies: These are laboratory-made proteins that attach to specific targets on cancer cells. They work like heat-seeking missiles, finding cancer cells by their unique surface markers and either blocking growth signals, marking the cells for destruction by your immune system, or delivering toxic substances directly to the cancer cell.
Examples: trastuzumab (Herceptin), rituximab, cetuximab, bevacizumab.
Small Molecule Inhibitors: These are drugs small enough to enter cancer cells and block specific enzymes or proteins that cancer needs to grow. Think of them as saboteurs that slip inside and disable critical machinery.
Examples: imatinib (Gleevec), erlotinib, vemurafenib, osimertinib.
Angiogenesis Inhibitors: These drugs starve tumors by blocking their ability to form new blood vessels. Tumors need blood vessels to grow beyond a certain size. Cut off their blood supply, and they cannot expand.
Examples: bevacizumab, sorafenib, sunitinib.
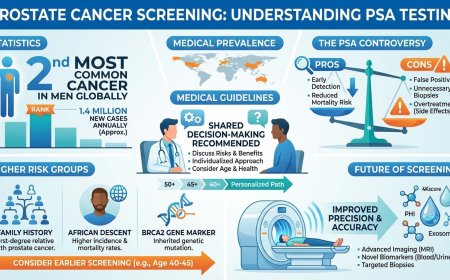
PARP Inhibitors: These drugs prevent cancer cells from repairing their damaged DNA, causing them to die. They work especially well in cancers with BRCA mutations.
Examples: olaparib, rucaparib, niraparib.
The Dangerous Excuses (And Why They Matter)
"I'm too overwhelmed to understand this right now."
Understandable. But your cancer isn't waiting for you to feel ready. Every week matters. Ask your oncologist to explain it in simple terms. Bring someone with you to appointments to help you process information.
"Targeted therapy sounds too complicated."
It doesn't have to be. You don't need to understand the molecular biology to make an informed decision. You just need to understand whether your tumor qualifies, what drug is recommended, and what the expected benefit is. Your oncologist can walk you through all of this.
"My cancer doesn't need it. Regular chemo will be fine."
This isn't about what you think your cancer "needs." It's about what the science shows. If your tumor has a targetable mutation and you skip the corresponding therapy, you're gambling with your life.
"I've heard it stops working after a while."
Some targeted therapies do eventually become less effective as cancer cells adapt. But "eventually" might mean years of good quality life. And when resistance develops, second-line targeted therapies are often available.
"I'm scared of the side effects."
Targeted therapies do have side effects. But compare:
Traditional Chemotherapy Side Effects: Severe nausea and vomiting, hair loss, extreme fatigue, mouth sores, and severe infections from low white blood cell counts.
Targeted Therapy Side Effects (vary by drug): Skin rashes, diarrhea, liver changes (usually manageable with monitoring), fatigue (generally milder than chemo), and drug-specific effects depending on the target.
Most patients on targeted therapy can continue working, maintain their hair, and live relatively normal lives during treatment.
Real Patient Story: Amit's Calculated Risk
Amit, a 58-year-old businessman from Delhi, was diagnosed with metastatic lung cancer with an EGFR mutation. His oncologist recommended osimertinib.
Amit's concern: "Doctor, I've read that people develop resistance to this drug. What's the point of starting something that will stop working?"
His doctor's response: "Without targeted therapy, median survival for your cancer stage is significantly shorter. With osimertinib, many patients live considerably longer, often with good quality of life. When resistance develops, we have other options. But right now, this gives you time you wouldn't otherwise have."
Amit started treatment four years ago. He's still playing golf twice a week, managing his business, and spending time with his grandchildren. Yes, his cancer may eventually become resistant. But those four years matter. They matter enormously.
The Questions You Must Ask Your Oncologist
When your doctor mentions targeted therapy, don't just nod. Ask:
"Has my tumor been tested for targetable mutations?" If not, ask why not. Biomarker testing should be standard for many cancer types.
"What specific mutation does my tumor have?" Understanding your cancer's molecular profile empowers you.
"What targeted therapy is recommended and why?" Get the specific drug name and the reason it matches your tumor.
"What are my chances with and without this therapy?" Ask for realistic information about recurrence risk and survival benefit.
"What are the side effects and how are they managed?" Understanding side effects helps you prepare and prevents panic when they occur.
"Are there biosimilar or generic versions available?" Ask about all available formulations of the recommended drug.
"What happens if this therapy stops working?" Plan ahead. Know what the backup options are.
"Is this covered by my insurance or are there patient assistance programs?" Financial planning is a legitimate part of cancer treatment planning.
Accessing Targeted Therapy in India
Targeted therapy drugs are available across India through several channels. Government cancer hospitals such as AIIMS, Tata Memorial Hospital, and regional cancer centres often provide access to these therapies, sometimes at subsidized rates. State government health schemes and national programs such as PM-JAY (Ayushman Bharat) may cover treatment at empaneled hospitals.
Biosimilar and generic versions exist for several targeted drugs and are approved for use in India, making many treatments more accessible than they were a decade ago. Manufacturer-run patient assistance programs are available for several drugs — contact the drug company directly to ask. Clinical trials at major cancer centres may also offer access to targeted therapies either free of charge or at reduced cost. NGOs such as CanKids and the Indian Cancer Society can provide guidance on navigating financial aid.
The question to ask is not whether you can access targeted therapy, but which pathway is most appropriate for your situation. Your oncologist and the hospital's medical social worker are your best starting points.
When Targeted Therapy Doesn't Work (The Reality You Need to Hear)
Targeted therapy isn't magic. It doesn't work for everyone.
Reasons It Might Not Work: Your tumor may not have a targetable mutation. Your specific mutation may not yet have a corresponding approved drug. Your cancer may develop resistance to the drug over time. Side effects may become intolerable in some cases. In rare instances, the drug simply does not work despite the mutation being present.
What Happens Then: This is not the end of the road. Your oncologist will try different targeted therapies if multiple options exist, switch to or add chemotherapy, consider immunotherapy, look at clinical trials for experimental drugs, or focus on controlling symptoms and maintaining quality of life.
The Difference Between Targeted Therapy and Immunotherapy (Stop Confusing Them)
Many patients mix these up. Here is the clear distinction:
Targeted Therapy attacks cancer cells directly by targeting specific mutations or proteins in the cancer. It works relatively quickly when it works, and typically stops working if you stop taking it.
Immunotherapy activates your immune system to attack cancer. It does not target specific mutations in most cases, may take months to show its effect, and can continue working even after treatment is stopped in some patients.
Both are forms of "precision medicine," but they work through completely different mechanisms. Some patients receive both simultaneously.
What to Expect During Targeted Therapy Treatment
Before Starting: Biomarker testing (results typically take two to three weeks), insurance approval or financial planning, baseline scans and blood tests, and a detailed discussion with your oncologist about the plan.
During Treatment: Most targeted therapies are pills taken daily at home. Some are IV infusions given every two to four weeks. Regular blood tests monitor organ function, and periodic scans check whether the cancer is responding. Side effects are managed as they arise.
Monitoring Response: The first scan typically occurs after two to three months. If working, treatment continues. If not working, the strategy is revised. If partial response, treatment continues with reassessment.
Living on Targeted Therapy: Most patients on targeted therapy continue working, maintain their daily routines, travel with proper planning, and avoid the severe debilitation often associated with aggressive chemotherapy regimens.
Real Patient Story: Deepa's Quality of Life
Deepa, a 45-year-old architect from Bangalore, has metastatic colon cancer with a BRAF mutation. She has been on a targeted therapy combination (encorafenib and cetuximab) for 18 months.
Her experience: "I take pills at home, get an IV infusion every two weeks, and go for scans every three months. I have skin rashes that I manage with creams, and occasional diarrhea. But I'm working on projects, traveling for site visits, and living my life. My friend who's on traditional chemo is hospitalized every cycle with infections and severe nausea. Same diagnosis, different treatment approach, completely different quality of life."
Deepa is earning, working, and living — not just surviving.
The Clinical Trials Option (Why You Should Consider It)
If targeted therapy for your specific mutation isn't available as standard treatment, clinical trials might be your answer.
What Clinical Trials Offer: Access to cutting-edge drugs not yet approved, often at no or reduced cost to the patient, close monitoring by expert oncology teams, and the potential for breakthrough results.
Risks: The drug might not work. There may be unknown side effects. More frequent hospital visits are required for monitoring. You may be in the control arm receiving standard treatment rather than the experimental drug.
Where to Find Clinical Trials in India: ClinicalTrials.gov (search by cancer type and location), Tata Memorial Centre clinical trials registry, AIIMS clinical trials, and major private cancer centres including Fortis, Apollo, and HCG.
The Conversation You Must Have Today
Stop procrastinating. Today, not tomorrow, take action.
If you've been diagnosed with cancer and haven't asked about biomarker testing, call your oncologist's office. Ask if your tumor has been tested for mutations. If not, ask why not.
If you've been told you have a targetable mutation but haven't started therapy, schedule an appointment to discuss the specific drug, the benefits, the risks, and all available access options.
If you're currently on targeted therapy and confused about monitoring, write down your questions and ask them at your next appointment. Don't leave until you understand.
If access to treatment is a concern, research patient assistance programs, contact the drug manufacturer, look into government health schemes, and explore clinical trials.
The Timeline That Matters
Early Action: Biomarker testing done at diagnosis. Treatment starts within four to six weeks. Best chance of controlling disease early. Fewer complications from delayed treatment.
Delayed Action (common scenario): Biomarker testing done months after diagnosis. Patient undergoes standard treatment that is less effective for their molecular subtype. Cancer progresses. Patient finally gets appropriate targeted therapy. Harder to control disease that has had time to advance. More intensive treatment required.
Every week counts. Cancer doesn't pause while you figure things out.
The Future Is Already Here
Targeted therapy isn't experimental. It's not fringe science. It's mainstream cancer treatment for those whose tumors qualify.
The future of cancer treatment is precision medicine — understanding the specific molecular profile of your cancer and attacking its specific vulnerabilities.
Are there guarantees? No. Cancer never comes with guarantees.
But if your tumor has a targetable mutation and a corresponding drug exists, choosing not to use it isn't caution — it's an unnecessary risk.
Your Life, Your Decision, Your Action
You have cancer. That's brutal and unfair and terrifying.
But if you're reading this, you have options. You have time to make decisions. You have the ability to advocate for yourself.
Don't let confusion become inaction. Don't let fear of the unknown keep you from potentially life-extending treatment. Don't let unanswered questions about access stop you from asking the right people the right questions.
Your oncologist mentioned targeted therapy for a reason. Find out what that reason is. Understand your tumor's mutations. Ask about corresponding drugs. Ask about every available access pathway.
This is not your fault. But it is your responsibility.
Every single day you delay getting answers is a day your cancer has free rein.
Call your doctor. Ask the questions. Get the information.
Your life is literally in your hands.
Professional Support Options
If you're experiencing possible cancer symptoms, seeking a second opinion, or unsure which tests or treatments are right for you, don't wait. Speak with a qualified oncologist today.
Connect with experienced U.S.-based cancer specialists for a comprehensive second-opinion consultation. They will carefully review your case and help determine the most appropriate next steps for your individual health needs:
👉 https://myamericandoctor.com/our-doctors/
You may also choose to enroll in our upcoming concierge medical clinic in India, Global Concierge Doctors. We offer U.S.-style primary care with 24/7 access to India-based physicians for ongoing guidance on any health concern. When required, we coordinate referrals to trusted specialists in India and the U.S. for advanced evaluation and care.
Your health decisions today shape your life tomorrow.
Reader Engagement
Quick Poll: Have you or a loved one been offered targeted therapy?
- Yes, and we started treatment
- Yes, but we're still deciding
- No, but we'd like to learn more
- I wasn't aware this was an option
Share This Article: If someone you know is navigating cancer treatment, share this information. Understanding targeted therapy could change their outcome.
Related Articles You Should Read:
- Understanding Biomarker Testing: Why Your Tumor's Genetic Profile Matters
- Chemotherapy vs. Targeted Therapy: What's Really Different?
- The Cost of Cancer Treatment in India: A Complete Financial Guide
- Clinical Trials Explained: When Standard Treatment Isn't Enough
Medical Disclaimer
This article is provided strictly for educational, informational, and awareness purposes only. It is not intended to be, and should not be construed as, professional medical advice, diagnosis, treatment, or a substitute for consultation with qualified healthcare professionals.
No Doctor-Patient Relationship
The information presented in this article does not establish a doctor-patient relationship between the reader and the author, publisher, or any affiliated entities. No medical decisions should be made based solely on the content of this article.
Consult Qualified Medical Professionals
If you are experiencing any symptoms mentioned in this article, have been diagnosed with cancer, or have concerns about cancer risk, seek immediate consultation with qualified oncologists, physicians, or appropriate medical specialists. For medical emergencies, contact emergency services immediately.
Individual Medical Situations Vary
Every person's medical condition, health history, risk factors, cancer type, and circumstances are unique. Diagnostic tests, treatment options, and medical recommendations must be tailored to individual patients through direct consultation with licensed healthcare providers who have access to complete medical histories and can perform proper clinical evaluations.
Not a Recommendation for Specific Tests or Treatments
References to biopsies, imaging studies (CT scans, PET scans, MRI), blood tests, tumor markers, chemotherapy, radiation therapy, immunotherapy, targeted therapy, surgery, or any other diagnostic procedures and treatments in this article are for informational purposes only and do not constitute recommendations that you should or should not undergo these tests or treatments. All decisions regarding medical testing, diagnosis, and treatment should be made in consultation with qualified healthcare professionals based on your specific medical situation.
No Guarantee of Accuracy or Completeness
While efforts have been made to provide accurate information, medical knowledge continuously evolves, particularly in the rapidly advancing field of oncology. The information in this article may not reflect the most current research, clinical guidelines, treatment protocols, or medical practices. The author and publisher make no representations or warranties regarding the accuracy, completeness, or timeliness of the content.
Do Not Disregard or Delay Professional Medical Advice
Never disregard, avoid, or delay obtaining professional medical advice from qualified healthcare providers because of something you have read in this article. If you have questions or concerns about information presented here, discuss them with your personal physician or oncologist. Early detection and prompt treatment significantly improve cancer outcomes.
Third-Party Resources and Links
Any references to third-party medical services, clinics, doctors, cancer centers, or external websites are provided for informational purposes only and do not constitute endorsements. The author and publisher are not responsible for the content, services, or practices of any third-party entities.
Limitation of Liability
To the fullest extent permitted by law, the author, publisher, and affiliated entities disclaim all liability for any direct, indirect, incidental, consequential, or punitive damages arising from the use of, or reliance on, information contained in this article. This includes, but is not limited to, medical complications, treatment decisions, or any other adverse outcomes.
Geographic and Regulatory Considerations
Medical regulations, standards of care, insurance coverage, availability of diagnostic tests, treatment protocols, and access to cancer therapies vary by country, region, and healthcare system. Information regarding procedures and medical practices may not be applicable to all geographic locations or healthcare settings.
Clinical Trials and Experimental Treatments
Any references to clinical trials, experimental treatments, or investigational therapies are for informational purposes only. Participation in clinical trials should only be considered after thorough discussion with your oncology team and a full understanding of all risks and benefits.
Your Responsibility
You acknowledge that you are solely responsible for your own health decisions and that you will consult with appropriate licensed healthcare professionals before making any medical decisions or undergoing any diagnostic tests or treatments.
Acknowledgment
By reading and using the information in this article, you acknowledge that you have read, understood, and agreed to this disclaimer in its entirety. You further acknowledge that this article has been created with the assistance of artificial intelligence. While every effort has been made to ensure accuracy, AI-generated content may occasionally contain errors, omissions, or inaccuracies. The information presented here is intended solely for educational and informational purposes and should not be relied upon as a substitute for professional medical advice. Readers are strongly encouraged to consult qualified healthcare professionals, refer to peer-reviewed medical literature, and cross-reference information from established clinical sources before making any health-related decisions.
Last Updated: 3rd February 2026
What's Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Angry
0
Angry
0
 Sad
0
Sad
0
 Wow
0
Wow
0